

The views expressed in our content reflect individual perspectives and do not represent the authoritative views of the Baha'i Faith.
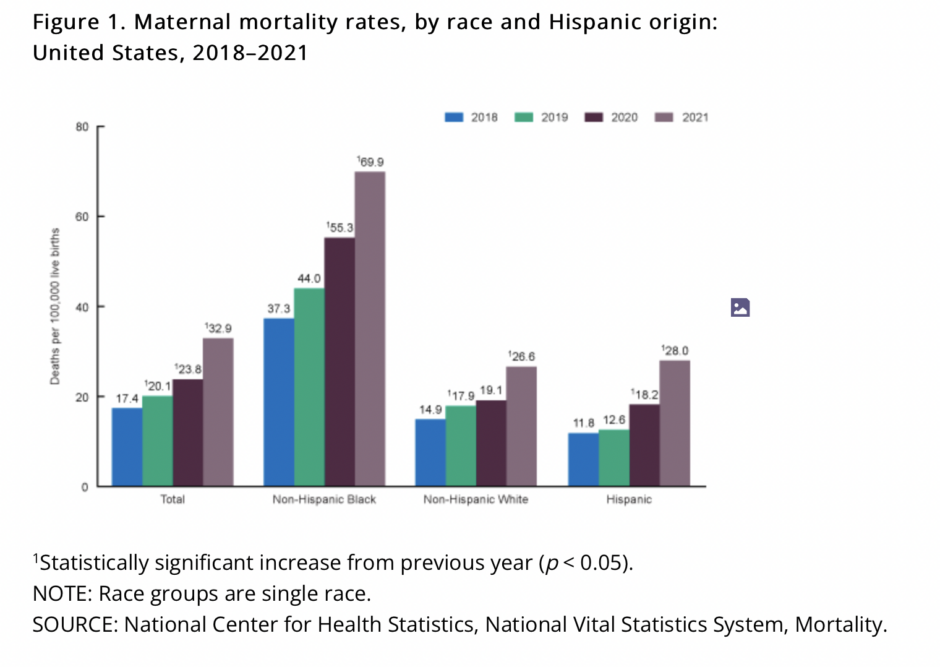
The 2021 maternal mortality rate in the United States was more than 10 times the estimated rates of many other high-income countries, including Australia, Austria, Israel, and Japan.
The U.S. maternal mortality rate has increased dramatically over the years, and due to structural and interpersonal racism and bias, Black women are dying more than every other race.
As the National Spiritual Assembly of the United States, the administrative governing body for the Baha’is in the U.S., wrote in “The Vision of Race Unity” in 1991:
A nation whose ancestry includes every people on earth, whose motto is E pluribus unum, whose ideals of freedom under law have inspired millions throughout the world, cannot continue to harbor prejudice against any racial or ethnic group without betraying itself. Racism is an affront to human dignity, a cause of hatred and division, a disease that devastates society.
Notwithstanding the efforts already expended for its elimination, racism continues to work its evil upon this nation. Progress toward tolerance, mutual respect, and unity has been painfully slow and marked with repeated setbacks.
My friend Karen VanKeuren, who is Black and white, experienced the same bias, neglect, and lack of respect that many Black women experience during childbirth when she had her second child in 1992.
She recalled, “I understood that walking would help with childbirth, so I walked in lieu of using a wheelchair to get to the emergency room. There were comments from the nurses and doctors basically deciding that I may have been dramatic. …I was told that my contractions weren’t hard enough, go home and wait, and come back later.”
But after she got home, her water broke and her son slipped into the birth canal.
Karen wrote, “My husband was not equipped to be of assistance to me at the time, and the situation was worsened because 911 wasn’t available where we lived. We called an ambulance, but it was going to take a while. Thankfully, I remembered a close friend who happened to be a field medic who lived quite close. He came to my house to help me discover my son was breech.
From there, after the ambulance arrived, thankfully, I was in excellent physical condition. I was able to push my son out because I had to do almost a stretch to touch my toes. Some medical equipment was knocked over, and my son and I remained connected for the ambulance ride.
When I arrived at the hospital, there was quite a bit of embarrassment from the physician and nurses that sent me home, and everybody went to tend to my newborn son, to ensure he was OK. I was left in the hallway for an extended period of time (at the time, I didn’t realize that if the placenta was still inside of me, I would still be having contractions). I just knew that I was still uncomfortable and pushed the placenta onto the floor in the hallway. All of this happened within one hour and 28 minutes.”
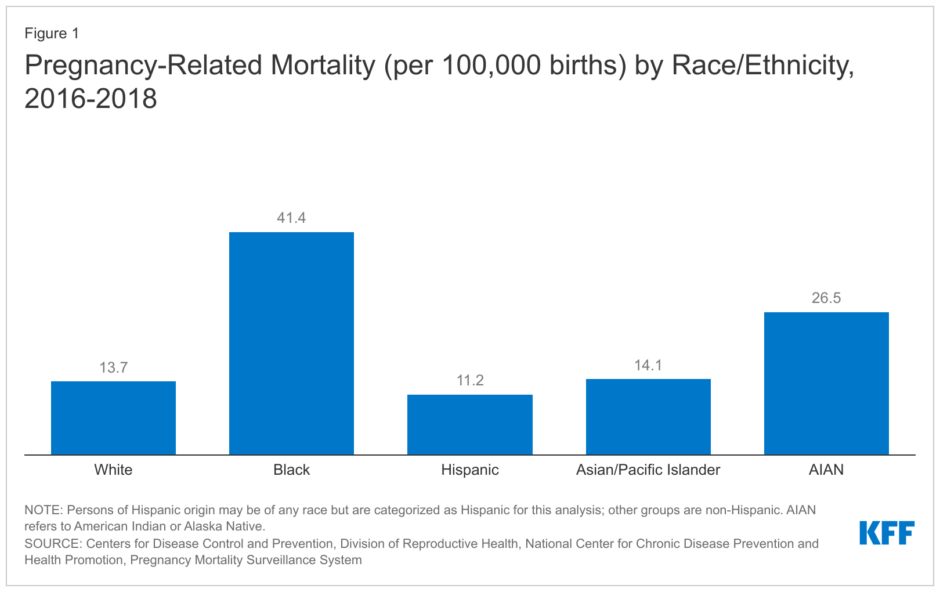
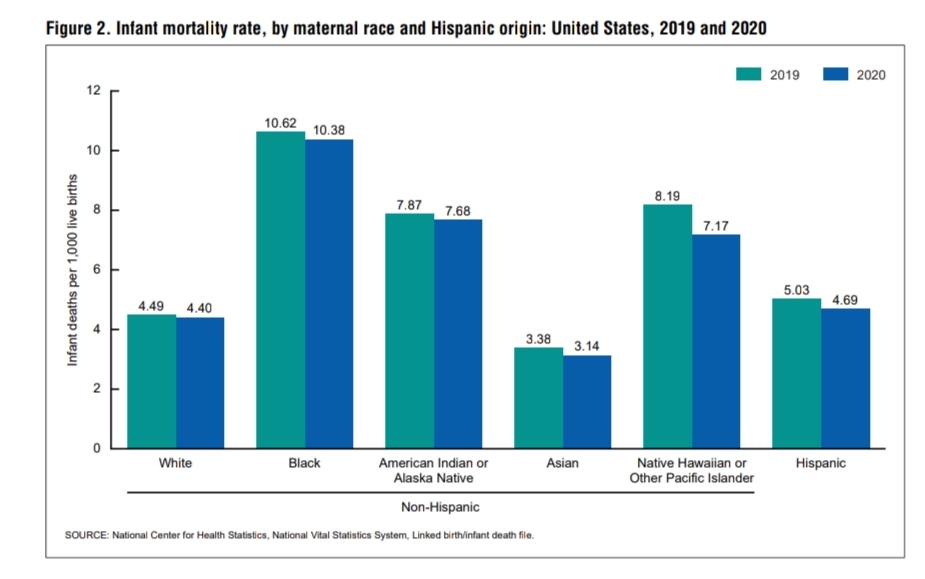
Fortunately, Karen had a friend who could help her deliver her baby after the hospital sent her away, and she and her son survived. Sadly, hundreds of women aren’t as lucky each year. The U.S. had one of the worst rates of maternal deaths in our nation’s history in 2021. And, according to the CDC, “Black women are three times more likely to die from a pregnancy-related cause than White women.”
The CDC also stated that “more than 80% of pregnancy-related deaths in the U.S. are preventable.” Since most maternal deaths are preventable, I reached out to Fatmata Williams, a community health education specialist and a registered nurse with twenty-seven years of diverse clinical and administrative experience, to learn how we can all help reduce Black maternal mortality in the U.S.
Be ye loving fathers to the orphan, and a refuge to the helpless, and a treasury for the poor, and a cure for the ailing. Be ye the helpers of every victim of oppression, the patrons of the disadvantaged.
Radiance Talley: Thank you, Fatmata, for taking the time to answer my questions. Since the majority of pregnancy-related deaths in the U.S. are preventable, what do doctors, nurses, and hospitals need to start doing to address Black maternal health disparities and prevent these deaths from happening?
Fatmata Williams: Maternal Mortality Review Committees identified the leading causes of maternal deaths: mental health (overdose, suicide, etc.) at 23%, excessive bleeding at 14%, cardiac and coronary conditions (relating to the heart) at 13%, infection at 9%, blood clots at 9%, cardiomyopathy (disease of heart muscle) at 9%, and hypertensive disorders at 7%.

These committees also highlighted that the leading causes of death differed based on race and ethnicity. Mental health conditions were the leading causes of death for Hispanic and Non-Hispanic White people, heart disease and associated conditions were the leading causes of death for Non-Hispanic Black people, excessive bleeding (hemorrhage) was the leading cause of death for Non-Hispanic Asian people, and mental health conditions and hemorrhages were the leading causes of death for American Indian and Alaska Native (AI/AN) people. When we know the underlying causes of death, we can do something to prevent the “preventable” deaths.
Preventing maternal deaths requires coordination and action steps at all levels (federal, state, county, town, hospital systems, group and private practices, communities, family, and individual). The C.D.C. Hear Her Campaign highlights critical interventions that can be implemented at each level to improve maternal health outcomes. Since a substantial percentage of U.S. births occur in hospitals, it is crucial to intervene at the hospital systems level to improve patient outcomes.
To this end, organizations like the Alliance for Innovation on Maternal Health (A.I.M.), in collaboration with the American College of Obstetrics and Gynecology (ACOG), have developed Patient Safety Bundles, a quality improvement initiative with several objectives to improve birthing practices and safety during childbirth which would improve patient outcomes and ultimately save lives. Hospitals across the country implement the A.I.M. safety bundles based on the needs of the population they serve. The value of the patient safety bundles lies in the improvements and consistency of safe care for all pregnant and postpartum people. Hospitals can also work with the Perinatal Quality Collaborative and the A.I.M. national team to learn about the process and receive technical and other support to implement their A.I.M. patient safety bundle of interest. Grant opportunities are available to aid hospitals in this process improvement initiative. The eight A.I.M. patient safety bundles are Obstetric Hemorrhage, Perinatal Mental Health Conditions, Sepsis in Obstetrical Care, Care for Pregnant and Postpartum People with Substance Use Disorder, Severe Hypertension in Pregnancy, Safe Reduction in Cesarean Section, Cardiac Conditions in Obstetric Care and Postpartum Discharge Transition.
Hospitals can also analyze data to see progress and care gaps, informing the next steps in their process improvement initiatives. Additionally, some hospitals nationwide have implemented implicit bias training for all their providers to raise awareness of the disparity in patient outcomes and highlight the roles that implicit bias and systemic and structural racism play in these poor outcomes for Black birthing people. Hospitals nationwide should also train all their staff on the national CLAS (culturally and linguistically appropriate services) standards in health and healthcare to improve service quality delivered to all individuals to reduce disparities and achieve health equity. Lastly, all hospitals should elicit patients’ feedback about their birthing experience before leaving. Each hospital leadership should boldly state the importance of soliciting the patient’s/family’s feedback to inform hospital policy. Hospitals should also promote shared decision-making for all patients, especially Black pregnant and postpartum people, and their families.
Radiance: What advice do you have for Black women to help them reduce their risk of dying during or after childbirth? Please include a few resources.
Fatmata: Black women and their families did not create this problem. Still, they can become a part of the solution by educating themselves about the scope of the problem, including things they can do to improve the situation. Some educational resources are available at the Black Mamas Matter Alliance and the Centers for Disease Control and Prevention websites. The C.D.C.’s “Hear Her Campaign” was explicitly designed to address the maternal mortality crisis. Black women must care for their physical and mental health before, during, and after pregnancy. They must plan their pregnancy, be aware of their medical/behavioral/social risk factors and inform their maternal health and primary care providers during consultation and treatment.
Black women and their families should be familiar with pregnancy, childbirth, and postpartum complications and communicate them effectively with the healthcare team. Black women and their families should know the pregnancy warning signs, including when to seek help. Black women and their families must learn to advocate for themselves and should feel empowered to change providers if they feel not listened to. Black women should plan ahead of time and be familiar with their maternity health insurance coverage to select services that may improve the birthing experience and maternal and birth outcomes. There is evidence that the use of prenatal/birth/postpartum doulas during pregnancy leads to a decreased Cesarean section (C-section) rate, lower premature birth rate, reduced low birthweight, decreased labor inductions, and other medical interventions, improved health in the newborn, increase breastfeeding and high patient satisfaction.
Unless it is medically necessary to protect the health of the mother, the baby, or both, Black women should not opt for a primary Cesarean section delivery. Even after a primary Cesarean section, Black women should get several medical opinions to explore the possibility of vaginal delivery after an initial C-section instead of opting for a C-section as the expected outcome. According to the March of Dimes, between 2017-2019, the overall U.S. C-section rate was high for first-time deliveries, and Black women had a higher C-section rate at 36.2 % compared to 30.8% for Non-Hispanic White women and 31.4 % for Hispanic women. C-section puts a woman at risk for post-surgical complications, possibly leading to poor health outcomes. Higher primary and secondary C-section rates for Black women put them at risk for poorer health outcomes than women of other races and ethnicities.
Black women and their families should educate themselves about pregnancy including the medically necessary reasons for C-sections. They should plan ahead of time for the appropriate delivery mode, including pain control. Black women and their families must question the motives for deviations in their treatment plans. They must assert themselves as active participants in their treatment. Finally, Black women and their families must build a support network. This support network is critical, especially for single parents to be. The postpartum period is also vital, especially to give the birthing parent some rest and to pay attention to their mental health. Postpartum blues, depression, psychosis, substance use overdose, suicide, infanticide, and intimate partner violence can all occur up to one-year postpartum. A good support network can identify these issues and get help for the woman to prevent adverse outcomes.
Radiance: How can everyone help reduce Black maternal mortality and support and advocate for the pregnant Black women in their lives?
Fatmata: People can support Black pregnant women in their lives by being present. Pregnancy is an exciting but very stressful time for any woman. However, for Black women, the stress is even more because of the fear and distrust of the healthcare system. Black women need a reassuring voice and support during pregnancy and postpartum.
Believe the Black women in your life when they tell you how they feel because they sometimes experience dismissal and a minimizing of their symptoms from the healthcare establishment. Educate yourself about pregnancy, including the warning signs to look for. Occasionally, you may notice a change before the pregnant person does. Be a part of the support network and provide support no matter how small you may think the support is.
Empower Black women to advocate for themselves and speak up when they feel something is wrong. If they believe something is wrong, they are the experts on their bodies. Encourage them to insist and assert themselves until they get help. It could save their lives. It is essential to be present every step of the way because if the woman is in a position where she cannot advocate for herself, you will be there to advocate for her. The key is to inform, empower, and advocate.

Radiance Talley serves as the director of operations at BahaiTeachings.org, where she integrates her expertise in SEO, journalism, design, and publishing into every aspect of her work. She has edited and written hundreds of articles for BahaiTeachings.org and has also written and optimized articles for...
READ MORE



Comments
Sign in or create an account
Continue with Googleor